 Ballooning due to the weakness of the muscle layer of a brain vessel is called a brain aneurysm. This ballooning causes weakening and thinning of the vessel wall. Bleeding into the brain tissue caused by rupturing of the vessel from the weak spot is called a subarachnoid hemorrhage. This type of bleeding can result in stroke, coma or even death.
Ballooning due to the weakness of the muscle layer of a brain vessel is called a brain aneurysm. This ballooning causes weakening and thinning of the vessel wall. Bleeding into the brain tissue caused by rupturing of the vessel from the weak spot is called a subarachnoid hemorrhage. This type of bleeding can result in stroke, coma or even death.
How is a brain aneurysm formed?
The exact cause of brain aneurysms are unknown. However, some factors are considered to contribute to aneurysm development. These factors are:
- Hypertension;
- Smoking;
- Genetic predisposition;
- Injured blood vessels;
- Some infections.
What happens if an aneurysm bleeds?
Not all aneurysms in the brain bleed. Sometimes, aneurysms leak through a small vessel tear. In that case the hemorrhage is less. Yet sometimes, the tear is large, which causes more serious symptoms, even death.
What are the treatment options in brain aneurysms?
Current treatment options are surgical (open brain surgery) and endovascular (clogging the balloon by entering the vessel from groin) treatment.
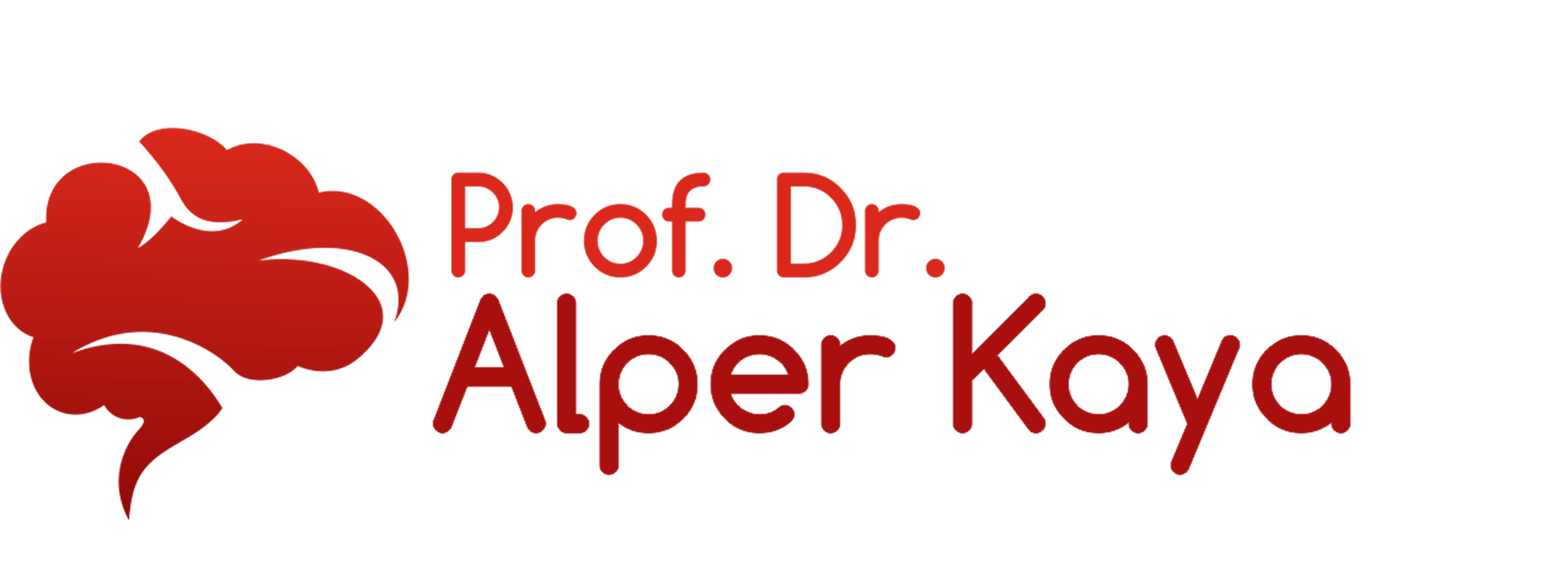
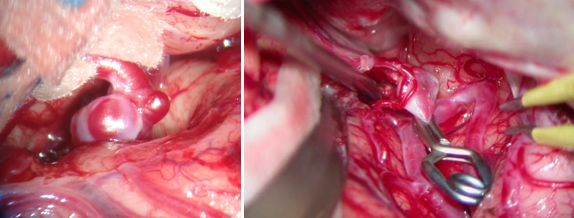
How is surgical treatment performed in brain aneurysms?
First “clipping” of brain aneurysms was performed in 1937. As the types of clips increased and microsurgical techniques were introduced to brain surgery in 1960s, surgical treatment has become the golden standard in brain aneurysms. Despite all advances, surgical clipping procedures are major and challenging operations.
Clipping is performed with craniotomy (removing a piece of the skull). Brain and brain vessels are reached through the opening of craniotomy and the aneurysm is located. Then, the aneurysm is carefully separated from the surrounding tissue and the aneurysm neck (base) is clipped with a small metal (usually titanium) clip. These clips have a coil mechanism and when placed they cut the blood flow into the aneurysm. The most valid and efficient method in the treatment of aneurysms is open surgical approach.
How is endovascular coiling (clogging the balloon) performed in brain aneurysms?
Use of endovascular techniques in the treatment of brain aneurysms was introduced in 1970s. The advances in the materials used in 1980s and approval of the technique in the US in 1995 facilitated its widespread use.
The aim of endovascular coiling is eradicating the aneurysm as in surgical clipping. The long-term indicator of treatment success is non-reappearance of the aneurysm. Re-opening of blood flow or growing of aneurysm is considered treatment failure.
A soft, platinum coil is used for the procedure. This coil is advanced up to the brain through a larger artery in the groin and is placed into the aneurysm. The coil inserted distorts the blood flow. A large blood clot forms due to the slowing blood flow. The clot clogs and closes the aneurysm, preventing it from rupture and bleeding. The long-term durability of endovascular coiling, which is more preferred in terms of intervention when compared to brain surgery in terms of intervention, is yet unknown. Also, not all aneurysms are suitable for coiling. If the balloon ruptures during the procedure, the patient usually dies. Sometimes, the clogging material can leak to normal circulation and clog intact vessels, which is a very serious complication. In addition, this technique is rarely preferred due to its high costs.
Who performs these treatments?
Brain surgeons perform surgical clipping. Endovascular coiling can be performed by brain surgeons or interventional radiologists.
What can be the side effects or risky situations that can be seen during these procedures? The most dangerous situation that can occur during both clipping and coiling is aneurysm rupture and intracerebral bleeding. Even though the exact rate is unknown, the risk is approximately 2-3% for both procedures. Ruptured aneurysm bleeds into the brain, which can lead to stroke, coma or death. Intervention of the ruptured aneurysm that can come up during both procedures is easier in open brain surgery, because the bleeding spot can be located and intervened more easily.
Stroke due to decreased blood flow and decreased oxygenation is another dangerous complication that can be seen in clipping and coiling. The extensity and distribution of the stroke depends on the location of the aneurysm.
The duration of the procedures, risks and how long it takes for the patients to go back to their normal lives depends on the location of the aneurysms, size of bleeding and medical condition of the patient. Every patient should be considered individually and these concerns should be discussed with the physician.


EMBOLIZATION (TREATMENT BY ENTERING THE VESSEL FROM GROIN)
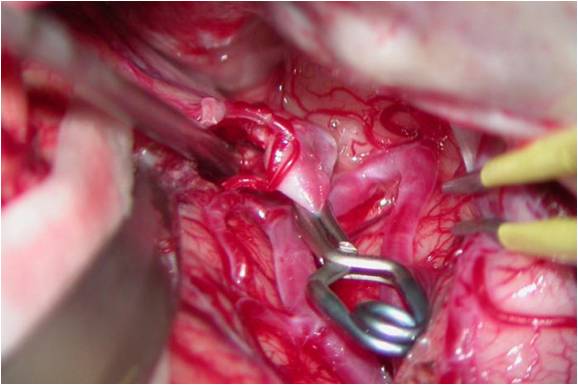

CLIPPING THE ANEURYSM (BALLOON) WITH BRAIN SURGERY